The sternoclavicular joint (SC joint) is a joint between the clavicle (collar bone) and the sternum (breastbone). It is a joint which transmits a reasonable amount of force during upper limb activities and has a moderate degree of rotation with arm motion.
Luckily, compared to most other joints in the upper limb the SC joint is much less frequently problematic. However, there are two uncommon issues which can be troublesome.
Sternoclavicular arthritis
In SC joint arthritic, most of the time the joint having a bulkier appearance but typically little in the way of pain.
However, infrequently pain can be problematic. Luckily for most people in this situation a steroid injection into the joint is effective in significantly relieving this pain.
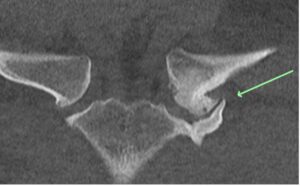
CT scan demonstrating arthritis of the SC joint on one side
However, if an injection fails to be sufficiently beneficial and if the symptoms are sufficiently bad surgery can be considered. Surgery can take the form of making a moderately long incision (cut) and remove about 5 mm of bone from the inner end of the clavicle. However, this is a relatively dangerous operation as behind the SC joint are some very large blood vessels which if injured can cause fatal bleeding.
To improve SC arthritis which has not responded sufficiently to steroid injections, I prefer to perform arthroscopic surgery using a small arthroscope to remove of part of the inner end of the clavicle with a burr. This form of surgery results in much smaller wounds, a more rapid recovery and is considerably safer than the open procedure.
Picture of SC arthroscopy occurring
Sternoclavicular joint instability
The SC joint can be dislocated typically by a significant force. It is a significant injury but rare injury. If an acute dislocation has occurred, it is best reduced in hospital as an emergency. If a dislocation becomes chronic it can be extremely difficult or impossible to type to improve this situation.
At times the joint can become unstable following a previous dislocation and there are procedures to reduce and stabilise the joint. This form of surgery is complex and not frequently performed but can take the form of tendon or implant reconstruction followed by a prolonged rehabilitation period.