
Instability & Dislocations
The extensive range of motion of the glenohumeral joint requires that the glenoid (socket of the shoulder) is shallow. For the shoulder to remain stable, it relies on the labrum cartilage to deepen the glenoid, the ligaments and capsule to offer further stability and for the rotator cuff muscles to centre the humeral head in the glenoid.
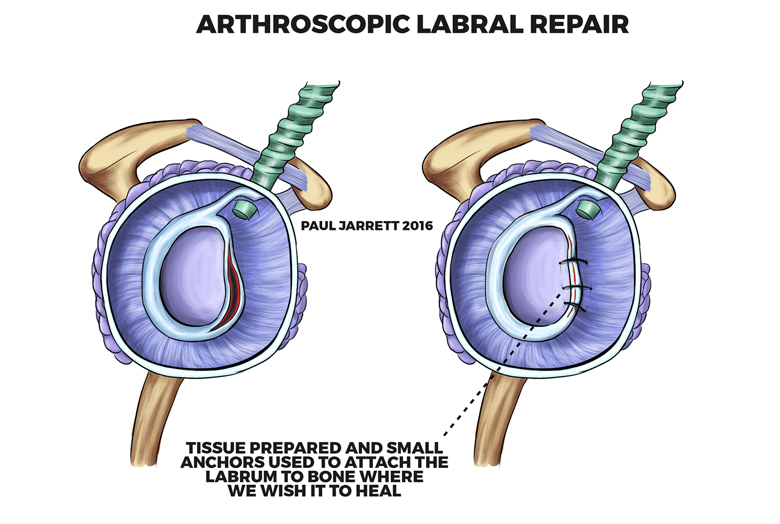
When the labrum and cartilage, and to a lesser extent the rotator cuff, are injured, shoulder stability can be reduced. When a shoulder dislocates, the structures that supported it in place are inevitably injured either in the form of stretching, but more commonly by tearing with or without stretching. It is common for the labrum to become detached from the glenoid (called a Bankart injury) occasionally with a degree of breaking (fracture) of the bone. Unfortunately, unlike some other joints, it is common for the injured structures to fail to heal in their original position, and therefore the shoulder can become unstable (chronic instability). Chronic instability is much more common in patients who dislocate their shoulder when young, especially in the late teenage years and early twenties. It can develop in older people, although it is less common. If your shoulder is unstable, you may experience symptoms such as your shoulder feeling like it is wobbly, or coming out of the joint throughout certain activities or positions of the shoulder, or it may actually dislocate during some activities. If the instability is minor, it is possible that all you will feel is pain and experience reduced function.How is shoulder instability treated?
Arthroscopic Labral Repair – Post-Operative Care
A sling is used following the operation for 4-6 weeks. For the first two weeks, most functions of the affected limb are restricted further by discomfort. I usually request a physiotherapist see you before admission to hospital, and/ or before discharge. From four weeks after the operation, it is possible to remove the sling and use your shoulder for light tasks, but heavy tasks must be avoided until 12 weeks after surgery. Returning to sport will depend upon your sport(s) and the level at which you participate, but in particular it is often required to avoid collision sports for up to 9 months following surgery.
You will be unable to drive for at least the first four weeks. This is to prevent injury to your repair site. Before you attempt to drive, you must gain sufficient comfort and upper limb control to drive safely under all conditions, and manage whatever events occur while driving. In practice, this usually takes at least six weeks after surgery and often considerably longer. It will be your decision when to return to driving, but you must have confidence that you are sufficiently capable of safe driving before you do so. No heavy activities are allowed until at least 12 weeks following your operation, even if your shoulder feels comfortable and has enough strength to do so.
You will require either no sutures or they will be absorbable. Some sutures may be internal and some external, but your wounds can be washed and moisturised from 10 days after your operation, and no dressings are required after this point. We have an aftercare video on our website which may assist with the removal of dressings, and a discussion of surgical risks in which Mr Jarrett would request you to read before your operation.