
Impingement & Bursitis
Shoulder impingement is characterised by pain in the shoulder usually going into the upper arm and often down towards your elbow.
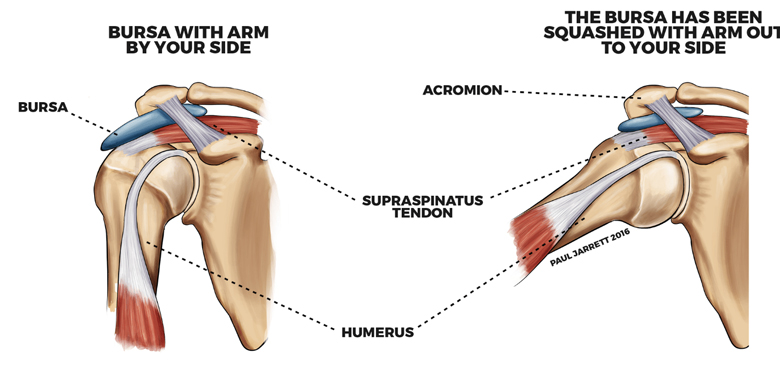
Shoulder motion is restricted principally on elevating the limb to the side. The pain often prevents you getting your hand behind your back. Lying on your affected shoulder at night often causes pain resulting in you waking. The symptoms can come on acutely for single, or several short, episodes. Episodes may become a recurring or constant problem. The subacromial space between the acromion and humeral head is narrowed when the shoulder is in certain positions. In subacromial impingement, the rotator cuff tendons and bursa tend to become swollen (often called bursitis). In the majority of people the undersurface of the acromion is flat (type I) but for some people the undersurface can be curved (type 2) or hooked (type 3) with type 2 and 3 acromions reducing the space available for the tendons and the bursa.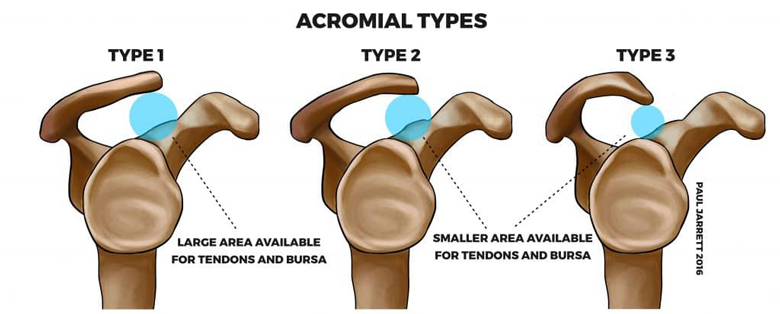
The subacromial space may be reduced due to a spur of bone on the front of the acromion, or a thickening of the coracoacromial ligament, or from the rotator cuff becoming less efficient at centring the gleno-humeral joint. Sometimes there may be some mild or modest fraying of the rotator cuff tendon (described as partial or full thickness tear on your ultrasound or MRI report) which may also result in the tendon being bulkier in the subacromial space.
As a result, the rotator cuff tendon and bursa compress in the space, and this causes pain. It is also possible for pain to come from other causes in addition to subacromial impingement such as rotator cuff tears or arthritis.
How is shoulder impingement / bursitis treated?
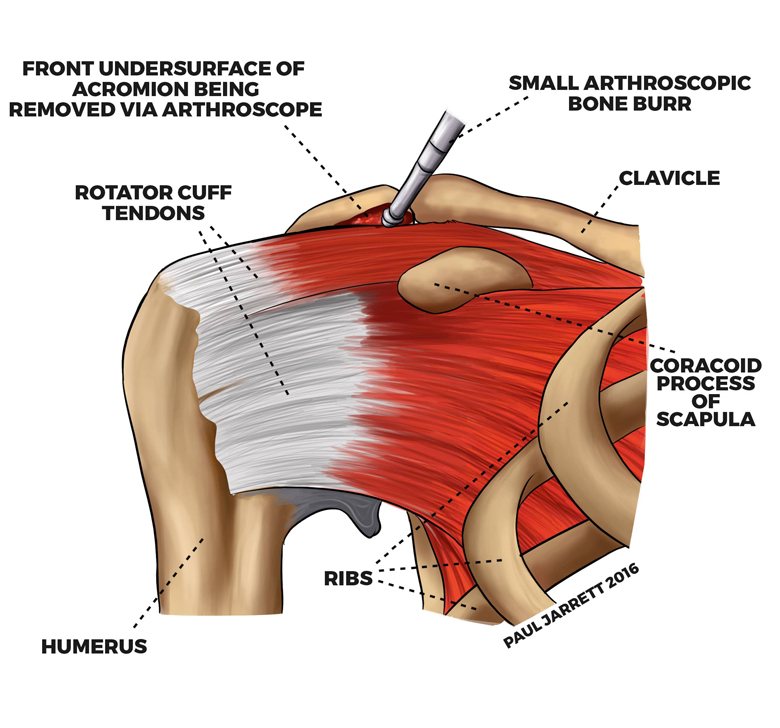
The operative procedure for elbow impingement / bursitis is called subacromial decompression or acromioplasty and is carried out under general anaesthetic. During the surgery, a portion of the undersurface of the acromion is removed to create sufficient room for the tendon.
Usually, this procedure is undertaken arthroscopically using an arthroscope (telescope) and small shavers (small surgical instruments designed to remove damaged or unwanted tissues) through three small cuts (incisions) around the shoulder.
The risks of this surgery include infection, prolonged stiffness, acromial fracture (rare), nerve and blood vessel injury (rare) and a failure to resolve symptoms.
Impingement/Bursitis
– Post-Operative Care
Patients usually spend one night in hospital following their subacromial decompression. No structures are repaired during this type of surgery. Therefore you can rehabilitate and use your shoulder as much as comfort allows. A sling can be worn for comfort, but its use is not essential. Mr Jarrett encourages you to reduce the use of the sling rapidly over a few days. Exercises are commenced immediately following the procedure.
Wound dressings are changed the day after your surgery, and all dressings can be removed 10 days postoperatively by yourself. You can then wash your skin including your wound as normal and moisturise your skin once or twice daily. It is unlikely you will have any sutures present but if any sutures have been used they will be absorbable. When you wash your shoulder over the next few days, they will fall out. There is a video on our website that may find helpful, with details on how to remove your dressings and what to expect after surgery.
Full recovery will take many months but most daily activities can usually be undertaken after 6 weeks, and by 3 months the shoulder should be sufficiently recovered to allow a majority of activities.